
Alberto Macin, mental health activities manager working with Doctors Without Borders/Médecins Sans Frontières (MSF) in Somalia, shares his experiences and explains how Somalia’s socio-economic and political challenges, and discrimination faced by vulnerable groups—especially women and children—lay the groundwork for mental health issues.
“Many women have experienced sexual violence, but it is something we cannot talk about.”
“I can no longer take care of my uncle. He has become very aggressive and has broken the chains we used to restrain him.”
“We have been displaced many times; hunger and poverty are now the only things we have left.”
“I don’t know how I can take care of him. They told me he also has psychosis. He can't do anything by himself, and I have to work to raise my children.”
“There is no hope left anymore ...”
These are some of the testimonies that my team and I have heard during mental health consultations with people in Galkayo and Baidoa districts of Somalia, where MSF works. Some of the issues we heard are related to violence, climate change, a lack of professional psychiatric services, chronic diseases, and extreme poverty.
Somalia, a nation burdened by decades of conflict, is no stranger to humanitarian crises. Amid the ravages of conflict, displacement, climate crises, and poverty, a mental health crisis looms large, affecting the lives of millions of people. Yet the mental well-being of those affected is often overlooked, resulting in a silent epidemic of psychological distress and disorders.
The mental health challenges in Somalia are closely intertwined with the nation’s socio-economic and political ones. Existing social problems and discrimination faced by vulnerable groups, especially women and children, lay the groundwork for mental health issues. This is compounded by natural disasters, prolonged conflict, and disease outbreaks, which bring additional layers of psychological trauma from family separation, lack of safety, the loss of livelihoods, and disrupted social territories. All of these contribute to acute emotional stress. In such environments, resources become scarce, further deepening the crisis.
The humanitarian response to the crises in Somalia, while often well-meaning, can also inadvertently exacerbate mental health problems. Overcrowding in camps, lack of privacy, and undermining traditional community support systems can heighten feelings of anxiety and insecurity among affected communities.

Years of conflict lead to stress disorders
The most common issues we see in Somalia include psychosomatic complaints, depression, stress, psychosis, and substance abuse. However, the stress of conflict also leads to new conditions or illnesses such as post-traumatic stress disorder (PTSD), bipolar disorder, types of anxiety, and acute stress reactions. For some people, the humanitarian [situation] can lead to hopelessness, particularly when basic needs like food, water, and access to health services are uncertain.
The World Health Organization (WHO) estimates that the prevalence of mental disorders among conflict-affected populations is 13 percent, with reports of mild forms of depression, anxiety, PTSD, bipolar disorder, and schizophrenia, while 4 percent experiences moderate forms of these disorders. Generally, women, elderly people, children, and people with disabilities are disproportionately affected by mental health issues. People with severe mental health disorders are especially vulnerable during emergencies, requiring both clinical care with medication and access to basic needs. However, these essential services remain out of reach for many. The story in Somalia is unfortunately no different.
In Somalia, MSF works in collaboration with the Ministry of Health, offering essential mental health care in Baidoa and Mudug. For us, mental health [intersects with] all medical activities. Teams provide psychosocial support, counseling, and specialized psychological care in health care facilities. However, the needs are many, and our services are not enough.
Currently, the Ministry of Health offers support and counseling to people living with HIV, tuberculosis (TB), and multi drug-resistant TB, focusing on chronic patients to reinforce adherence and have an impact on quality of life. Some local organizations provide mental health services for survivors of sexual, psychological, social and economic violence. While there are great efforts made by Ministry of Health and local organizations, it is not enough. Many people who require pharmaceutical and psychological treatment to recover functionality and integrate into their usual activities are left out of the loop.
Responding to mental health needs in Somalia
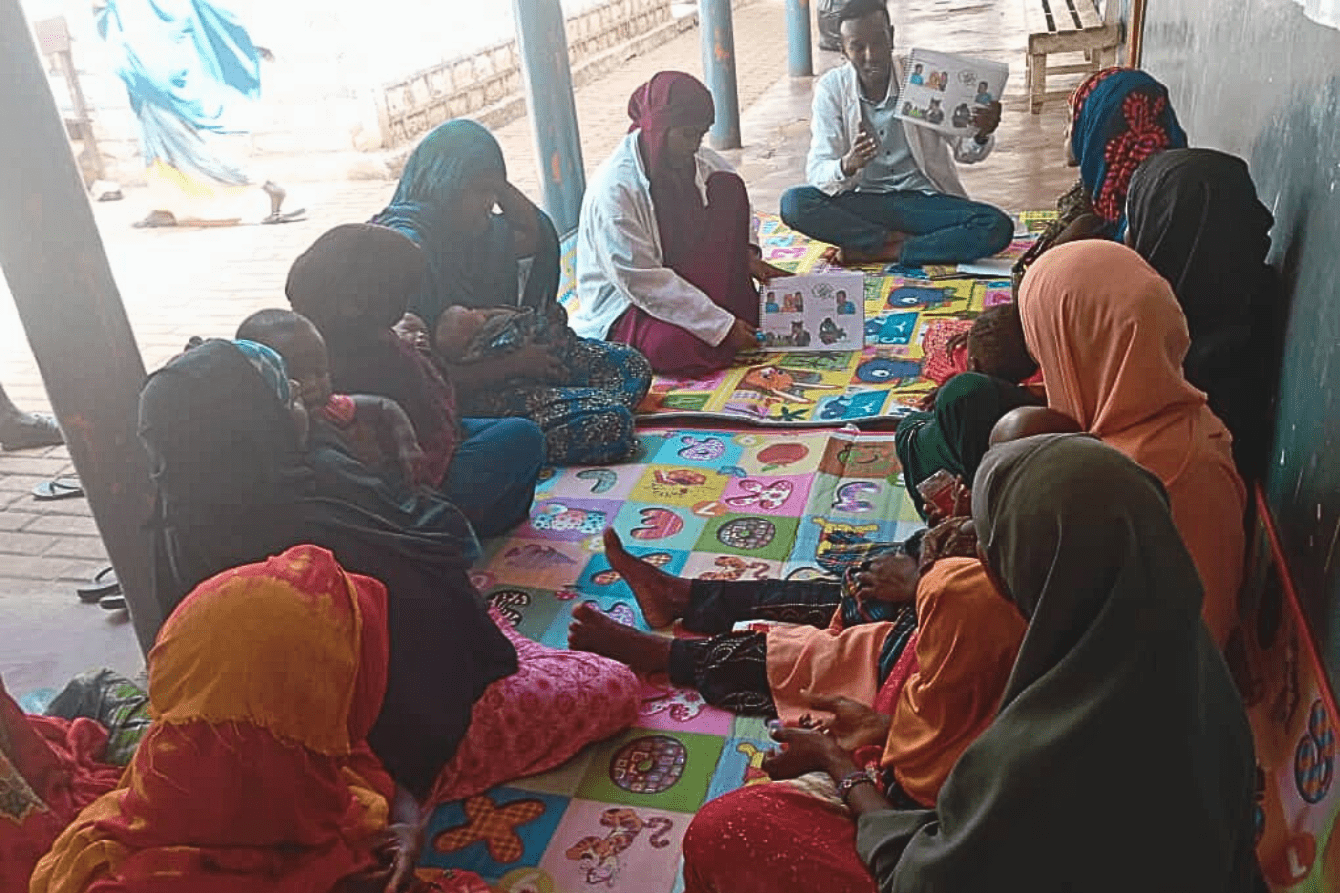
Between January and September 2024, MSF’s mental health teams working in Somalia have conducted a total of 4,940 mental health consultations. Additionally, we conducted 7,644 group activities for mental health and psychological education; promotion of healthy coping strategies; training for community leaders, health care workers, and non-medical teams in the management of psychological first aid; and peer support. [Our activities have reached] a total of 38,476 people. The mental health needs of communities are enormous, but the scale remains invisible. Lack of funding for mental health services, a lack of trained health care workers and supplies, limited data and scientific research, and a fractured health system have all worsened the problem.
Addressing mental health in Somalia requires an immediate and coordinated response. Clinical care for mental health must be integrated into broader humanitarian efforts, promoting the coverage of basic needs such as food, safe spaces, shelter, basic mental health support like psychological first aid, community awareness, psychosocial groups, recreational activities, and clear referral pathways to secondary mental health services. Mental health specialists, such as psychiatric nurses, psychologists, and psychiatrists should oversee mental health services, ensuring access to quality care.
Somalia’s communities—resilient despite the adversity they face—must be empowered to take an active role in mental health support. Strengthening community self-help and social support systems will help address the needs of people in the absence of clinical specialists. By creating or re-establishing community groups, Somalis can collectively solve problems and offer psychological support to those suffering. This social cohesion not only restores a sense of normalcy but also provides emotional relief to those affected by the crisis.

Mental health is an integral part of first response
Psychological first aid should be a key component of emergency response efforts. Trained workers, including health staff, teachers, and volunteers, should offer emotional and practical support to those in distress. These interventions, while seemingly small, can make a significant difference in the early stages of trauma.
Failing to address this pressing issue will only perpetuate the cycle of suffering. Now is the time for humanitarian agencies, local authorities, and the international community to prioritize mental health care, ensuring that it is fully integrated into the broader emergency response. In doing so, we can offer hope and healing to the millions of Somalis whose mental well-being hangs in the balance.
Somalia’s future depends not just on rebuilding its infrastructure, but on healing the minds and hearts of affected people.



